- coronary (adj.)
- c. 1600, “suitable for garlands,” from Latin coronarius “of a crown,” from corona “crown” (see crown (n.)). Anatomical use is 1670s for structure of blood vessels that surround the heart like a crown. Short for coronary thrombosis it dates from 1955. Coronary artery is recorded from 1741.
Anesthetic Considerations for Coronary Artery Disease patients, from Open Anesthesia
General:
- avoid swings: keep normotensive (20% baseline) and baseline HR
- Closely watch I/O EKG as 1mm ST change (+/-) for >60s = 10x cardiac event risk
- 5 mins of hr >105 = 10x death risk p/o
Imaging/Studies
- Assess echo, stress tests, viability studies, cath for LV fx, valve abnormalities, CAD
- Quick Guide images:
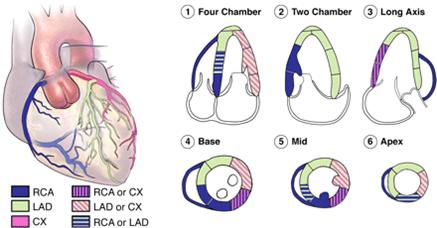
Distribution of Coronary Arteries in relation to Echo Segments 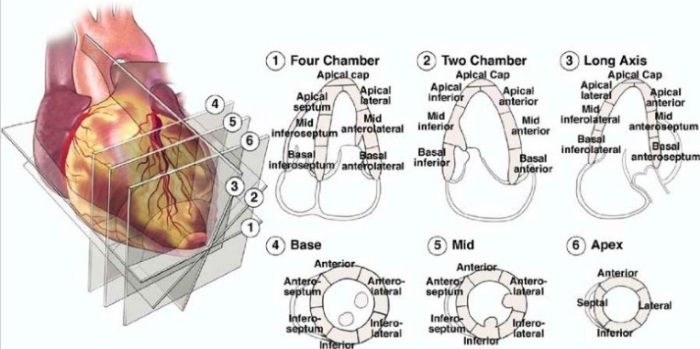
Echo Segments and 3D View
Starting Off: Induce and Intubate
- Etomidate or low dose propofol, Fentanyl + Midazolam
- DL < 15s (be quick!)
- if anticipate difficult intubation, consider spraying lidocaine, blocks, or iv lido prior to DL
Keep it going: Maintenance and Monitoring
- Debate between Volatiles vs. N20 Opiate, conflicting data, use judgement
- Volatiles depress but also provide preconditioning that is helpful
- Short acting BB (Esmolol) not proven to help, but use judgement
- Paralytics: Pancuronium increases BP and HR, Atracurium and miv can lower BP, Vec/Reoc/Cis neutral (though some concern about histamine with Cis, much lower than Atracurium)
- Don’t reverse: glyco not well tolerated
- Standard cardiac setup if high risk surgery (cardiac) or high risk pt (recent MI, CHF, unstable angina)
- NTG good for ischemia
Finish up: Avoid hypothermia, adequate analgesia and sedation en route to ICU
